
Eating disorders are complex mental illnesses characterized by persistent disturbances in eating and eating-related behaviours that result in harm to one’s physical health, mental health, and/or psychosocial functioning. These behaviours often serve as ways of coping with distressing life circumstances, interpersonal difficulties, and/or negative emotions. Eating disorder behaviours may also be symptoms of malnourishment or starvation, and/or can be a response to a difficult, stressful, or traumatic situation. You can learn more about the different types of eating disorders under Eating Disorders & Treatment.
While you will need to see a doctor, nurse practitioner, or psychologist in order to get a diagnosis, we have two different screening tools that can help you identify whether your thoughts, feelings, and behaviours relating to food, eating, and/or your body are consistent with symptoms of an eating disorder:
1. Screen for Disordered Eating (PDF)
Important note: These are not diagnostic tools and not substitutes for a professional evaluation.
Eating concerns occur on a continuum that encompasses behaviours such as constantly worrying about our body shape and what we eat, as well as clinical eating disorders, like anorexia nervosa or bulimia nervosa. The development of an eating disorder can be the result of a combination of genetic, environmental, and psychological causes. This is referred to as the biopsychosocial model. Risk factors include:
Some people do not meet the criteria for a diagnosable eating disorder, but experience eating disorder symptoms that negatively impact their lives. If this describes you, it’s still worth thinking about how you can access support.
Eating disorders are serious illnesses, but people can – and do – recover fully.
Recovery looks and feels different for everyone. For some, it is an ongoing process of healing. For others, being recovered means they feel like they can live a full and satisfying life. Many people fully recover to the point where they no longer struggle with disordered thoughts, feelings, and behaviours related to food and their body.
It can definitely be scary and overwhelming to realize there may be a concern and to actually reach out for help. Feeling conflicted about “recovery” or “healing” is very normal regardless of where you are in your journey. It doesn’t invalidate the small or large part of you that is worried and/or wants something to change.
Frustration, exhaustion, and impatience are all common in the recovery experience. The healing process can be very lengthy and include multiple lapses or relapses. Having a support system can help reduce isolation, empower you with skills and strategies for coping with intense emotions and challenging settings, and strengthen your resilience and capacity for self-compassion. Consider this web of support a guide for various components you could tap into to build a support system.

There is no right or wrong approach. Click through the next header(s) under "How Can I Get Support?" for more information on what support could look like
It can be difficult to speak openly and constructively about your needs with friends and family if you’re struggling with food and weight issues. Perhaps you had a bad experience in the past or you’re scared they won’t understand – those are all valid concerns. However, if you often find yourself stuck in uncomfortable situations, such as conversations focused on food, weight, and dieting, letting your loved ones know about your struggle can be a step towards creating safer and more neutral spaces conducive to your recovery.
Although being open about your experience can be a frightening thing to consider, it can also be an empowering action to take. For tips on starting a conversation, read the section, “How to tell someone I’m struggling”.
Self-directed resources, like educational videos, blog posts, workbooks, and support apps (e.g. Recovery Record) can be good starting points for learning more about disordered eating and practical strategies. Check out NEDIC’s list of coping strategies for some ideas. If you’d like specific suggestions for resources that may be useful in your given situation, connect with us on our helpline and/or live chat service.
Peer support and online groups can be a good resource for those who feel isolated and would like to connect with others who have had similar experiences. Community-based groups are often free or low-cost and many can be accessed without a diagnosis or referral. Many are also drop-in groups, meaning you don’t have to worry about committing to something you’re not sure will be a good fit. Groups offer opportunities for participants to share experiences, realize that they aren’t alone in their feelings, and help each other deal with difficulties they are facing.
Going to a primary care provider (e.g. family doctor or nurse practitioner) is a great first step because they are medically qualified to provide you with an assessment and diagnosis. They can also refer you to a specialized eating disorder program for further assessment and treatment. If you don’t have a primary care provider, you can go to a walk-in clinic.
The two resources below can help guide the conversation with your primary care provider and ensure that they have enough information to properly assess your health and determine the appropriate diagnosis in case they don’t have training in eating disorders. Unfortunately, not all primary care providers have this training; however, many are open to learning in order to support patients. The Guide for Primary Care Providers was developed for this reason.
Patient Checklist (PDF)
Guide for Primary Care Providers (PDF)
Getting a diagosis can be difficult for multiple reasons, including biases among health care providers. Some health care providers unfortunately have beliefs that prevent them from recognizing eating disorders beyond the stereotype of anorexia nervosa in thin teenaged girls or young women. For some individuals, getting a diagnosis involves a great deal of persistence, advocating for themselves, and consulting multiple health care providers.
While a diagnosis is not required to access all treatment options, most publicly-funded services are limited to individuals who have been diagnosed by a health professional.
Keep in mind that you don't need to meet all of the criteria for an eating disorder diagnosis to deserve help. If you are struggling with disordered eating, seek support.
An initial assessment with a primary care provider (who could be a family doctor, general practitioner, or nurse practitioner) can help determine the kind of support that is most appropriate for your situation. Primary care providers can monitor your health and, where appropriate, provide a referral to a provincially-funded eating disorder treatment program or to specialists for diagnosis and care.
NEDIC maintains a Service Provider Directory, which contains listings of service providers across Canada that have expertise in eating disorders, ranging from publicly-funded treatment clinics, to community-based organizations, to professionals in private practice. You can search the directory for options that you can access from your location. You can also call or chat with us – we can search the directory for you and refer you to relevant service providers. Many offer telephone or online services. You can also use this tip sheet to help decide if a provider suits your needs.
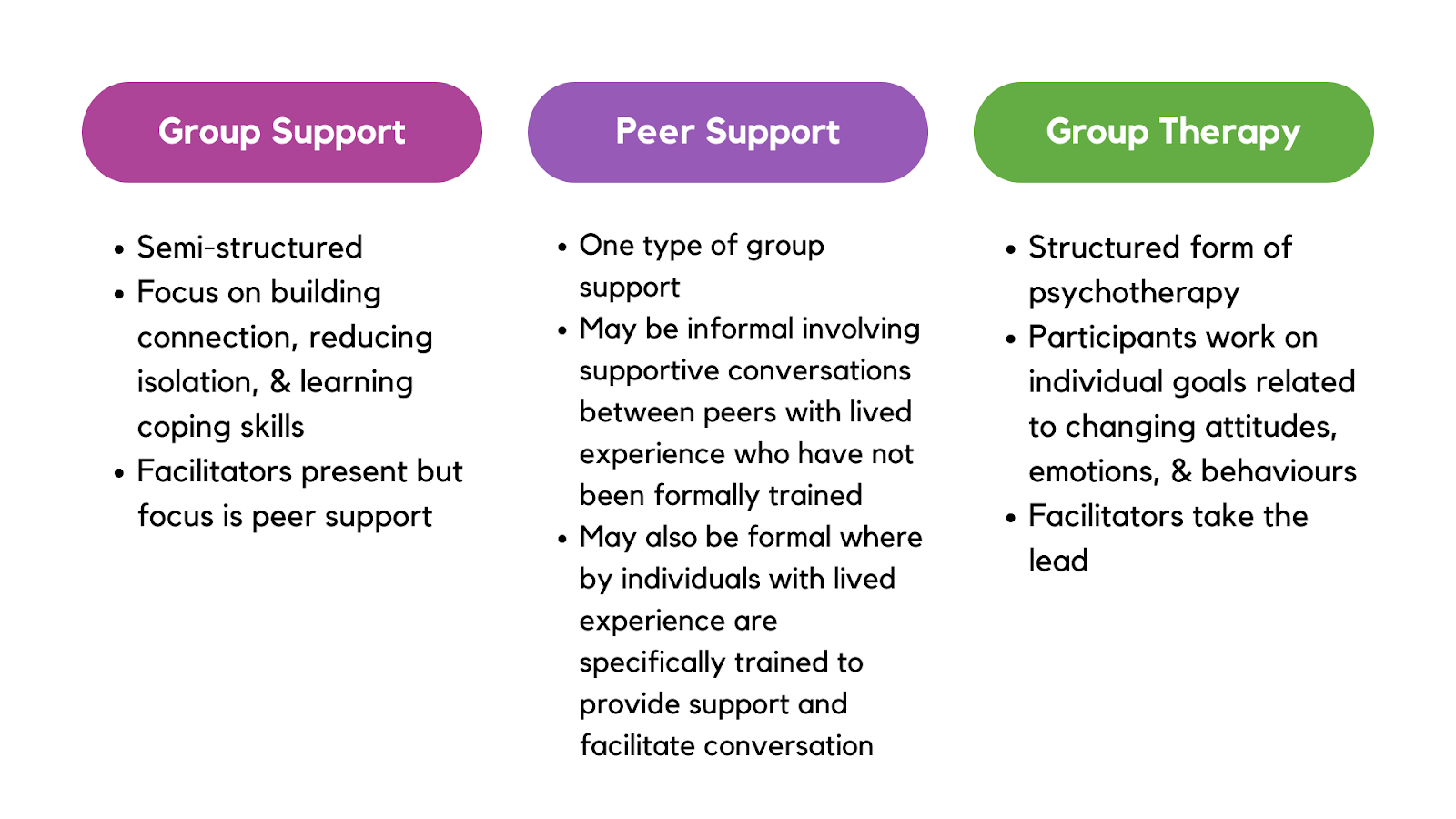
Group therapy and support. Support groups allow group members to hear from other people who might be having similar experiences in a space where a trained facilitator is present to assist with group safety and reduce harm. Group assistance often helps to reduce isolation, enhance connection, and facilitates psychoeducation and opportunities for skill-building.
Individual counselling or therapy. This may be appropriate for individuals who feel overwhelmed in groups or who feel that they would benefit more from one-on-one attention. Individual mental health services may be provided by a therapist, a psychologist, a social worker, or a counsellor, or a psychiatrist. Dietitians also offer specialized nutrition counselling which may benefit individuals experiencing eating disorders. The majority of individual services that exist for eating disorders are provided by professionals in private practice, and therefore have fees attached. Private or extended health benefits plans can at least partially cover the costs of these services. You can read about the different types of providers who offer individualized support under Eating Disorders & Treatment.
Provincially-funded eating disorder treatment programs. These are generally run out of hospitals. There are multiple levels of care – inpatient, day hospital, outpatient. Intensive treatment programs in Canada (i.e. inpatient and day hospital) are concentrated in the biggest urban areas. Services are facilitated by a multidisciplinary team of professionals. Access to these programs often require a doctor’s referral. Read more about this under Eating Disorders & Treatment.
People whose eating problems have reached a stage of medical and/or psychological crisis are often guided to seek more intensive support. This might include hospitalization or other specialized treatment programs within a hospital or community agency, which may require a doctor's referral.
The physical and psychological signs and symptoms listed below are some of the indicators of the need for immediate medical attention, such as calling an ambulance, visiting the emergency room, or if available, accessing a mobile crisis team. Please note that the list below is not exhaustive and that the items that appear here aren’t necessarily in order of increasing severity, but a given combination of signs and symptoms may mean that an individual is in particular danger.
These situations can be extremely overwhelming and challenging to navigate, whether you’re personally experiencing an eating disorder or you’re trying to support someone who is. NEDIC’s helpline and live chat services are not equipped to provide intensive support in cases where conditions such as the above are present. If you or a person you are supporting is in an extremely high-risk situation, we advise you to access immediate medical attention through a visit to your nearest emergency room, medical clinic, or contacting a crisis-specific mental health helpline such as those offered by Talk Suicide Canada or your local community option.
It can be frustrating when resources are limited or hard to find. The amazing thing about support is that it comes in so many forms in different places. Services are available across Canada, even virtually. Help is still an option.
We can help figure out what is available to you. Connect with a trained support worker through our anonymous and confidential helpline and/or instant chat service, and we’ll walk you through your care options. Read our blog post What Can the Helpline Do for Me? for more information.
If you’d like to explore options on your own, check out the online community groups offered across Canada and use our service provider directory to find local and/or virtual options.
Tip! When using the service provider directory, make sure to select online services and use the filter button on the top right corner of the results page to broaden the distance of your search. Under the "Accessibility" heading, you can select services that are open to residents of your province/territory as well as to residents across Canada.
The healthcare system for youth can look different than what’s available for adults. For example, as the recommended first-line treatment for youth with eating disorders in hospitals is an outpatient approach known as Maudsley/Family-Based Therapy, parents or guardians are often more involved in the treatment process. For more about Maudsley Therapy, please visit "types of treatment"
Teenagers often (rightfully) worry about how much of a “say” they will get when it comes to deciding next steps for help. As a minor, your participation in medical decision-making really depends on the healthcare provider’s assessment of whether you’re developmentally capable of understanding the nature and consequences of your medical concern and the expected risks and benefits of the proposed treatment. Keep in mind that everyone’s developmental growth happens at different rates and it’s largely determined by biological factors (i.e. genetics).
If you’re in a situation wherein the healthcare provider has recommended and decided to involve your parents/guardians in the decision-making process, this doesn’t mean that you can’t still advocate for your needs and preferences or make your thoughts known (i.e. what’s working, what’s not, your fears, where you want support, etc.). Ultimately, if you reach out to a healthcare provider privately first, it may be helpful to ask about their policies on confidentiality and how involvement with adults could look like in case it’s necessary.
If you’re worried that your parents/caregivers won’t understand or take you seriously, sometimes seeking a private appointment with the healthcare provider can help with ensuring you are safe in the meantime and allows you space and time to work with your support options to prepare for the conversation with your parents/guardians. Consider sharing NEDIC's Caregiver's Guide with them to see if it helps answer their questions, and know that people supporting you can connect with our helpline and live chat services if they’d like to talk with us anonymously and confidentially.
Try to identify a safe person
Look for someone you trust – they could show signs of being patient, non-judgemental, and open to listening.
While the person you identify might not know much about disordered eating during your initial conversation, we trust that if they’re someone you trust, they are someone who genuinely cares for you and would be open to looking at resources, learning more about how to support you.
Prepare for the conversation
Finding a way to organize your thoughts can help in making the conversation as comfortable as possible. You could prepare by writing down what you want to say and how you’d like the conversation to flow. It might be helpful to think about:
For more ideas on how to break down your experience – the physical, emotional, and social changes – you can fill out our Patient Checklist and use it as a guide for identifying areas of concern you’d like to talk about. It’s important to highlight that the disordered behaviours are not just impacting you physically, but also mentally. This can help the person you’re talking with to better understand the scope of the effect of the disordered eating.
If you’re thinking of having a conversation in-person, you could refer to your notes to help guide the chat or even read it aloud. If it feels too scary or unsafe to say this aloud, you could pass over your notes for the person to read, or consider sending them an e-mail or text. If you express yourself better orally, but face-to-face communication feels a bit too vulnerable, you could try speaking over the phone. Ultimately, remember you have lots of options. Choose what works for you and how you think you’ll have the most productive conversation.
What if they react poorly/dismiss my concerns?
It can hurt and be extremely discouraging when you gather your courage to tell someone about your concerns and they don’t provide you with the support you hoped for and need. Know that if this happens, it’s not your fault and it doesn’t invalidate your worthiness for help and treatment. It also doesn’t mean that you were wrong to share.
Since disordered eating behaviours are often normalized and glorified or outright shamed in our society, many people lack knowledge and awareness when it comes to this topic. They may not know how to react when someone first shares their concerns with them, and are afraid of saying the wrong thing. It doesn’t mean that the doors are completely shut – sometimes people just need some time to process their fear, denial, or confusion, before being able to respond with support. Letting them know about NEDIC could help them connect with resources or a trained support worker to learn more about eating disorders and how they, as a safe person you’ve identified, can help you.
Sometimes the responses are well-intended, but fueled by misconceptions about eating disorders. You’re allowed to let them know what is helpful and what isn’t. Ultimately, you deserve support now, and if it seems like they’re not listening to you, it’s not your responsibility nor is it fair for you to spend so much time and energy to provide psychoeducation to convince someone.
Structuring the conversation
Deciding to connect with a primary care provider can be a good first step. If you currently have one, consider disclosing your concerns with them and planning for next steps (e.g. a medical referral to an outpatient program or to a nutritionist). If you don’t have a primary care provider at the moment and instead are looking for walk-in options, is there someone, like a friend or family member, who could recommend a doctor they’ve seen before for mental health concerns?
Opening up by asking your parents/caregivers for help, possibly giving up some aspects of control, can be scary and make you hesitate. That’s valid! We included this section because many young people find it easier to navigate their healing journey when they have social support around them. The following tips are just suggestions and may not necessarily apply to your situation nor be an approach you’re comfortable with. Take what you need and leave the rest.
Self-validation: Before and after conversation
Vulnerability is hard – it takes a lot to open up about this, and even harder when the disordered eating voice may tell you not to. Practicing self-validation is important as it can be helpful in building self-acceptance and a better understanding of our own internal experience, thoughts, and feelings.
Engaging in self-validation before and/or after telling your parents/caregivers may help you feel more aware and grounded in your thoughts and feelings, which often helps with managing intense emotions.
Some examples of self-validating statements you could say aloud or write out:
We also recognize that self-validation often requires self-compassion which can be hard for some of us. Know that you’re not alone. If you’re struggling to practice self-validation, reach out to us on the helpline or chat. We can act as a sort of a pre-call or debrief for your conversation with your parents/caregivers.
If you’re living with other people, such as a partner or room/housemates, it’s important to figure out what and how much you want to disclose to them about your situation. It can be helpful to set boundaries around the kind of support you’re asking for and that they are capable of providing.
To gain a sense of how a housemate may react and whether they’d be open to supporting you and/or learning more, you could leave articles around the house or bring up in passing, stories on eating disorders you’ve heard on the news or through social media, that talk about eating disorders and/or body image.
Taking the first step to open up the conversation can be the hardest. If you normally text with your housemate, you might feel less vulnerable (and more brave) if the conversation around disclosing the eating disorder or asking for support took place over text while you were still in the same room (perhaps sitting next/across each other in the living room). It can allow you some space and possible buffers (e.g. the TV), but make it easy for physical connection, eye contact, and reassurance if needed. Alternatively, you could ask to chat while sitting back-to-back if face-to-face communication is intimidating or anxiety-provoking.
If you’ve disclosed to your housemate you’re struggling with an eating disorder / disordered eating, you can set boundaries on how to best talk about this concern within the home, such as creating rules to address frequency, timing, typical support vs. emergency responses, etc. For example: